

Facts and Statistics
Key information to help better understand food allergy and anaphylaxis.
FARE works on behalf of the millions of Americans who have food allergy, including those at risk for life-threatening anaphylaxis. This page includes important facts and statistics that can help you better understand food allergies and anaphylaxis.
Works Cited
1 NIAID-Sponsored Expert Panel. Guidelines for the diagnosis and management of food allergy in the United States: Report of the NIAID-sponsored expert panel. J Allergy Clin Immunol. 2010; 126(6):S1-58.
2 Warren CM, Chadha AS, Sicherer SH, Jiang J, Gupta RS. Prevalence and Severity of Sesame Allergy in the United States. JAMA Network Open 2019; 2(8):e199144. DOI: 10.1001/jamanetworkopen.2019.9144.
3 Davidson L, Jones B. The Racial and Ethnic Makeup of Food Allergy Immunotherapy Trials. J Allergy Clin Immunol. 2021 147(2), Feb. 1, 2021 Supplement, Abstract 93.
4 Mahdavinia M, Fox SR, Smith BM, James C, Palmisano EL, Mohammed A, Zahid Z, Assa’ad AH, Tobin MC, Gupta RS. Racial Differences in Food Allergy Phenotype and Health Care Utilization Among US Children. J Allergy Clin Immunol Pract. Mar-Apr 2017;5(2):352-357.e1.
5 Warren C, Lei D, Sicherer S, Schleimer R, Gupta R. Prevalence and characteristics of peanut allergy in US adults. J Allergy Clin Immunol. June 2021; 147(6): 2263-2270.E5.
6 U.S. Food and Drug Administration. Food Allergen Labeling and Consumer Protection Act of 2004 (FALCPA). Updated March 7, 2022. https://www.fda.gov/food/food-allergensgluten-free-guidance-documents-regulatory-information/food-allergen-labeling-and-consumer-protection-act-2004-falcpa. Accessed May 20, 2022.
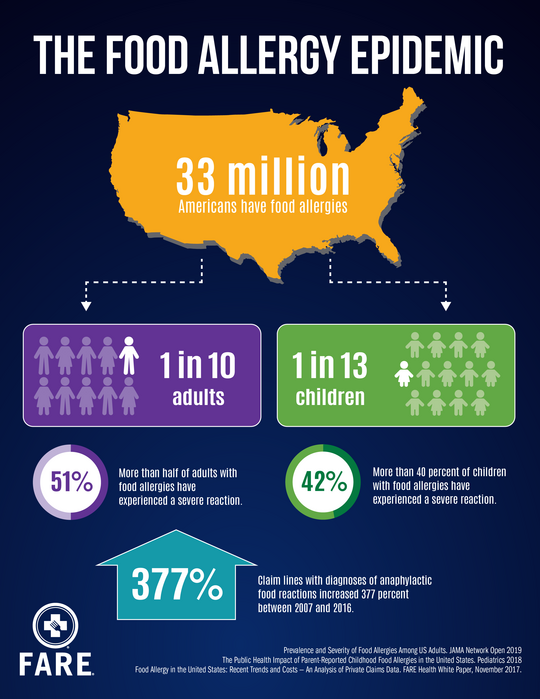
7 Gupta RS, Warren CM, Smith BM, Jiang J, Blumenstock JA, Davis MM, Schleimer RP, Nadeau KC. Prevalence and Severity of Food Allergies Among US Adults. JAMA Network Open 2019; 2(1):e185630.doi:10.1001/jamanetworkopen.2018.5630.
8 U.S. Census Bureau. Age and Sex Composition in the United States: 2022. Retrieved from https://www.census.gov/data/tables/2022/demo/age-and-sex/2022-age-sex-composition.html on September 7, 2023.
9 Gupta RS, Warren CM, Smith BM, Blumenstock JA, Jiang J, Davis MM, Nadeau KC. The Public Health Impact of Parent-Reported Childhood Food Allergies in the United States. Pediatrics 2018; 142(6):e20181235.
10 Zablotsky B, Black LI, Akinbami LJ. Diagnosed allergic conditions in children aged 0–17 years: United States, 2021. NCHS Data Brief, no 459. Hyattsville, MD: National Center for Health Statistics. 2023. DOI: https://dx.doi.org/10.15620/cdc:123250.
11 Jackson KD, Howie LD, Akinbami LJ. Trends in allergic conditions among children: United States, 1997-2011. NCHS data brief, no 121. Hyattsville, MD: National Center for Health Statistics. 2013. Retrieved from http://www.cdc.gov/nchs/products/databriefs/db121.htm.
12 Sicherer SH, Muñoz-Furlong A, Godbold JH, Sampson HA. US prevalence of self-reported peanut, tree nut, and sesame allergy: 11-year follow-up. J Allergy Clin Immunol. 2010; 125(6):1322-1326.
13 Keet CA, Savage JH, Seopaul S, Peng RD, Wood RA, Matsui EC. Temporal trends and racial/ethnic disparity in self-reported pediatric food allergy in the United States. Ann Allergy Asthma Immunol. 2014 Mar; 112(3):222-229.
14 U.S. Department of Education, Office for Civil Rights. Questions and Answers on the ADA Amendments Act of 2008 for Students with Disabilities Attending Public Elementary and Secondary Schools. https://www2.ed.gov/about/offices/list/ocr/docs/dcl-504faq-201109.html. Accessed May 20, 2022.
15 Gupta R, Holdford D, Bilaver L, Dyer A, Holl JL, Meltzer D. The economic impact of childhood food allergy in the United States. JAMA Pediatr. 2013 Nov; 167(11):1026-31.
16 Bilaver LA, Kanaley MK, Fierstein JL, Gupta RS. Prevalence and Correlates of Food Allergy Among Medicaid-Enrolled United States Children. Acad Pediatr. Jan-Feb 2021;21(1):84-92.
17 American Academy of Allergy, Asthma and Immunology, and American College of Allergy, Asthma and Immunology. Joint Task Force on Practice Parameters; Joint Council of Allergy, Asthma and Immunology. The diagnosis and management of anaphylaxis: an updated practice parameter. J Allergy Clin Immunol. 2005; 115:S483-523.
18 Bock SA, Muñoz-Furlong A, Sampson HA. Further fatalities caused by anaphylactic reactions to food, 2001–2006. J Allergy Clin Immunol. 2007; 119(4):1016-1018.
19 Bock SA, Muñoz-Furlong A, Sampson HA. Fatalities due to anaphylactic reactions to foods. J Allergy Clin Immunol. 2001; 107(1):191-193.
20 Sampson HA, Mendelson L, Rosen J. Fatal and near-fatal anaphylactic reactions to food in children and adolescents. N Engl J Med.1992; 327(6):380-384.
21 Korenblat P, Lundie MJ, Danker RE, Day JH. A retrospective study of epinephrine administration for anaphylaxis: how many doses are needed? Allergy Asthma Proc. 1999; 20:383-386.
22 Sampson HA. Anaphylaxis and Emergency Treatment. Pediatrics 2003; 111(S6):1601 -1608.
23 Ellis AK, Day JH. Incidence and characteristics of biphasic anaphylaxis: a prospective evaluation of 103 patients. Ann Allergy Asthma Immunol. 2007 Jan; 98(1) 64-69.
24 Shemesh E, Annunziato RA, Ambrose MA, Ravid NL, Mullarkey C, Rubes M, Chuang K, Sicherer M, Sicherer S. Child and parental reports of bullying in a consecutive sample of children with food allergy. Pediatrics 2013; 131:e10-e17.
25 Herbert L, Shemesh E, Bender B. Clinical management of psychosocial concerns related to food allergy. J Allergy Clin Immunol Pract. 2016; 4(2):205-213.
26 Bollinger ME; Dahlquist LM, Mudd K; Sonntag C, Dillinger L, McKenna K. The impact of food allergy on the daily activities of children and their families. Ann Allergy Asthma Immunol. 2006; 96:415-421.
27 Walker SO, Mao G, Caruso D, Hong X, Pongracic JA, Wang X. Cardiovascular risk factors in parents of food-allergic children. Medicine (Baltimore). 2016 Apr; 95(15): e3156.
28 Gupta RS, Springston EE, Smith B, Warrier MR, Pongracic J, Holl JL. Geographic variability of childhood food allergy in the United States. Clin Pediatr (Phila). 2012; 51(9):856-861.
29 McGowan EC, Bloomberg GR, Gergen PJ, Visness CM, Jaffee KF, Sandel M, O'Connor G, Kattan M, Gern J, Wood RA. Influence of early-life exposures on food sensitization and food allergy in an inner- city birth cohort. J Allergy Clin Immunol. 2015; 135(1):171-178.
30 Liacouras CA, Furuta GT, Hirano I, Atkins D, Attwood SE, Bonis PA, Burks AW, Chehade M, Collins MH, Dellon ES, Dohil R, Falk GW, Gonsalves N, Gupta SK, Katzka DA, Lucendo AJ, Markowitz JE, Noel RJ, Odze RD, Putnam PE, Richter JE, Romero Y, Ruchelli E, Sampson HA, Schoepfer A, Shaheen NJ, Sicherer SH, Spechler S, Spergel JM, Straumann A, Wershil BK, Rothenberg ME, Aceves SS. Eosinophilic esophagitis: Updated consensus recommendations for children and adults. J Allergy Clin Immunol. 2011 Jul; 128(1):3-20.
31 Kamdar TA, Peterson S, Lau CH, Saltoun CA, Gupta RS, & Bryce PJ. Prevalence and characteristics of adult-onset food allergy. J Allergy Clin Immunol Pract. 2015; 3(1):114–115.e1.
32 Ford LS, Taylor SL, Pacenza R, Niemann LM, Lambrecht DM, Sicherer SH. Food allergen advisory labeling and product contamination with egg, milk, and peanut. J Allergy Clin Immunol. 2010; 126(2):384-385.
33 Hefle SL, Furlong TJ, Niemann L, Lemon-Mule H, Sicherer S, and Taylor SL. Consumer attitudes and risks associated with packaged foods having advisory labeling regarding the presence of peanuts. J Allergy Clin Immunol. 2007; 120:171-176.
34 Taylor SL, Baumert JL. Cross-contamination of foods and implications for food allergic patients. Curr Allergy Asthma Rep. 2010 Jul; 10(4):265-70.
35 Simonte SJ, Sonhui M, Shideh M, Sicherer S. Relevance of casual contact with peanut butter in children with peanut allergy. J Allergy Clin Immunol, 2003; (112):180-182.
36 Wainstein BK, Kashef S, Ziegler M, Jelley D, Ziegler JB. Frequency and significance of immediate contact reactions to peanut in peanut-sensitive children. Clin Exp Allergy. 2007; 37(6):839–845.
37 Crespo JF, Pascual C, Dominguez C, Ojeda I, Munoz FM, Esteban MM. Allergic reactions associated with airborne fish particles in IgE-mediated fish hypersensitive patients. Allergy. 1995; 50(3):257-61.
38 Roberts G, Golder N, Lack G. Bronchial challenges with aerosolized food in asthmatic, food-allergic children. Allergy. 2002; 57:713-7.
39 Furlong TJ, DeSimone J, Sicherer SH. Peanut and tree nut allergic reactions in restaurants and other food establishments. J Allergy Clin Immunol. 2001; 108:867-870.
40 Sicherer SH, Furlong TJ, DeSimone J, Sampson HA. Self-reported allergic reactions to peanut on commercial airliners. J Allergy Clin Immunol. 1999; 103(103):186-189.
41 Comstock SS, DeMera R, Vega L, Boren EJ, Deanne S, Haapanen LA, Teuber SS. Allergic reactions to peanuts, tree nuts, and seeds aboard commercial airliners. Ann Allergy Asthma Immunol. 2008; 101:51-56.
42 Greenhawt MJ, McMorris MS, Furlong TJ. Self-reported allergic reactions to peanut and tree nuts on commercial airlines. J Allergy Clin Immunol. 2009; 124(3):598-599.
43 Nowak-Wegrzyn A, Conover-Walker MK, Wood RA. Food-allergic reactions in schools and preschools. Arch Pediatr Adolesc Med. 2001; 155(7):790-795.
44 Sicherer SH, Furlong TJ, DeSimone J, Sampson HA. The US peanut and tree nut allergy registry: characteristics of reactions in schools and day care. J Pediatr. 2011; 138(4): 560-565.
45 White MV, Hogue SL, Bennett ME, Goss D, Millar K, Hollis K, Siegel PH, Wolf RA, Wooddell MJ, Silvia S. EpiPen4Schools pilot survey: Occurrence of anaphylaxis, triggers, and epinephrine administration in a U.S. school setting. Allergy Asthma Proc. 2015 Jul-Aug; 36(4):306-312.
46 McIntyre CL, Sheetz AH, Carroll CR, Young MC. Administration of epinephrine for life-threatening allergic reactions in school settings. Pediatrics 2005; 116(5):1134-1140.
47 DeSantiago-Cardenas L, Rivkina V, Whyte SA, Harvey-Gintoft BC, Bunning BJ, Gupta RS. Emergency Epinephrine Use for Food Allergy Reactions in Chicago Public Schools. Amer J Prev Med. 2015; 48(2): 170-173.
48 Hefle SL, Taylor SL. Allergenicity of edible oils. Food Technol. 1999; 53:62-70.
49 Laoprasert N, Wallen ND, Jones RT, Hefle SL, Taylor SL, Yunginger JW. Anaphylaxis in a milk-allergic child following ingestion of lemon sorbet containing trace quantities of milk. J Food Prot. 1998; 61:1522-1524.
50 Gern JE, Yang E, Evrard HM, Sampson HA. Allergic reactions to milk-contaminated nondairy products. N Engl J Med. 1991; 324:976-979.
51 Yunginger JW, Gauerke MB, Jones RT, Dahlberg MJE, Ackerman SJ. Use of radioimmunoassay to determine the nature, quantity and source of allergenic contamination of sunflower butter. J Food Prot. 1983; 46:625-628.
52 Jones R, Squillace D, Yunginger J. Anaphylaxis in a milk-allergic child after ingestion of milk contaminated kosher-pareve-labeled “dairy-free” dessert. Ann Allergy. 1992; 68:223-227.
53 Hourihane J, Kilbrun S, Nordlee J, et al. An evaluation of the sensitivity of subjects with peanut allergy to very low doses of peanut: a randomized, double-blind, placebo-controlled food challenge study. J Allergy Clin Immunol. 1997; 100:596-600.
54 Bush RK, Taylor SL, Nordlee JA, Busse WW. Soybean oil is not allergenic to soybean-sensitive individuals. J Allergy Clin Immunol. 1985; 76:242-245.
55 Taylor SL, Busse WW, Sachs M, Parker JL, Yunginger JW. Peanut oil is not allergenic to peanut - sensitive individuals. J Allergy Clin Immunol. 1981; 68:372-375. 56 Hoffman DR, Collins-Williams C. Cold-pressed peanut oils may contain peanut allergen. J Allergy Clin Immunol. 1994; 93:801-802.
57 Keating MU, Jones RT, Worley NJ, Shively A, Yunginger JW. Immunoassay of peanut allergens in food-processing materials and finished foods. J Allergy Clin Immunol. 1990; 86:41-44.
58 Crevel RW, Kerkhoff MA, Koning MG. Allergenicity of refined vegetable oils. Food Chem Toxicol. 2000;38(4):385-393.
59 U.S. Food and Drug Administration. Food allergen labeling and consumer protection act of 2004 (public law 108-282, title II). Retrieved from http://www.fda.gov/food/labelingnutrition/FoodAllergensLabeling/GuidanceComplianceRegulatoryIn formation/ucm106187.htm
60 Perry TT, Conover-Walker MK, Pomes A, Chapman MD, Wood RA. Distribution of peanut allergen in the environment. J Allergy Clin Immunol. 2004; 113(5):973-976.
61 Du Toit G, Roberts G, Sayre PH, Bahnson HT, Radulovic S, Santos AF, Brough HA, Phippard D, Basting M, Feeney M, Turcanu V, Sever ML, Gomez Lorenzo M, Plaut M, Lack G for the LEAP Study Team. Randomized trial of peanut consumption in infants at risk for peanut allergy. New Engl J Med. 2015; 372:803-813.
62 Togias A, Cooper SF, Acebal ML, Assa'ad A, Baker JR, Beck LA, Block J, Byrd-Bredbenner C, Chan ES, Eichenfield LF, Fleischer DM, Fuchs GJ, Furuta GT, Greenhawt MJ, Gupta RS, Habich M, Jones SM, Keaton K, Muraro A, Plaut M, Rosenwasser LJ, Rotrosen D, Sampson HA, Schneider LC, Sicherer SH, Sidbury R, Spergel J, Stukus DR, Venter C, Boyce JA. Addendum guidelines for the prevention of peanut allergy in the United States: Report of the National Institute of Allergy and Infectious Diseases–sponsored expert panel. J Allergy Clin Immunol. 2017; 39(1):29-44.
63 Du Toit G, Sayre PH, Roberts G, Sever ML, Lawson K, Bahnson HT, Brough HA, Santos AF, Harris KM, Radulovic S, Basting M, Turcanu V, Plaut M, Lack G for the Immune Tolerance Network LEAP-On Study Team. N Engl J Med 2016; 374:1435-1443.
64 Lanser BJ, Wright BL, Orgel KA, Vickery BP, Fleischer DM. Current Options for the Treatment of Food Allergy. Pediatr Clin North Am. 2015; 62(6):1531-1549.
65 Wood RA. Food allergen immunotherapy: Current status and prospects for the future. J Allergy Clin Immunol. 2016; 137(4): 973-982.
66 Kim EH, Yang L, Ye P, Guo R, Li Q, Kulis MD, Burks AW. Long-Term Sublingual Immunotherapy for Peanut Allergy in Children: Clinical and Immunologic Evidence of Desensitization. J Allergy Clin Immunol. 2019; 144(5): 1320-1326.
67 Fleischer DM, Greenhawt M, Sussman G, Bégin P, Nowak-Wegrzyn A, Petroni D, Beyer K, Brown- Whitehorn T, Hebert J, Hourihane JO’B, Campbell DE, Leonard S, Chinthrajah RS, MD12, Pongracic JA, Jones SM, Lange L, Chong H, Green TD, Wood R, Cheema A, Prescott SL, Smith P; Yang W, Chan, ES, Byrne A, Assa’ad A, Bird JA, Kim EH, Schneider L, Davis CM, Lanser BJ, Lambert R, Shreffler W. Effect of Epicutaneous Immunotherapy vs Placebo on Reaction to Peanut Protein Ingestion Among Children With Peanut Allergy: The PEPITES Randomized Clinical Trial. J Am Med Assoc. 2019; 321(10):946-955.children and young adults. J. Allergy Clin Immunol. 2017; 139(4):1242-1252.
68 FAIR Health. Food Allergy in the United States: Recent Trends and Costs – An Analysis of Private Claims Data. FARE Health White Paper, November 2017. https://collections.nlm.nih.gov/catalog/nlm:nlmuid-101751558-pdf. Accessed February 14, 2023.
69 FDA approves first drug for treatment of peanut allergy for children. U.S. Food and Drug Administration. January 31, 2020. https://www.fda.gov/news-events/press-announcements/fda-approves-first-drug-treatment-peanut-allergy-children. Accessed February 14, 2023.
70 U.S. Food and Drug Administration. FASTER Act Video for Food Industry and Other Stakeholders. Updated January 31, 2022. https://www.fda.gov/food/cfsan-constituent-updates/faster-act-video-food-industry-and-other-stakeholders. Accessed May 20, 2022.
71 American Academy of Allergy, Asthma & Immunology. Anaphylaxis Defined. Allergy, Asthma & Immunology Glossary. https://www.aaaai.org/Tools-for-the-Public/Allergy,-Asthma-Immunology-Glossary/Anaphylaxis-Defined. Accessed February 14, 2023.
72 Bilaver LA, Kester KM, Smith BM, Gupta RS. Socioeconomic Disparities in the Economic Impact of Childhood Food Allergy. Pediatrics. 2016;137(5):e20153678.
73 Zablotsky B, Black LI, Akinbami LJ. Diagnosed Allergic Conditions in Children Aged 0-17 Years: United States, 2021. NCHS Data Brief. 2023 Jan;(459):1-8. PMID: 36700870. https://www.cdc.gov/nchs/products/databriefs/db459.htm
74 Jerschow E, Lin RY, Scaperotti MM, McGinn AP. Fatal anaphylaxis in the United States, 1999-2010: temporal patterns and demographic associations. J Allergy Clin Immunol. 2014 Dec;134(6):1318-1328.e7.
75 Lieberman J, Sublett J, Ali Y, Haselkorn T, Damle V, Chidambaram A, Rosen K, Mahr T. Increased Incidence and Prevalence of Peanut Allergy in Children and Adolescents in the United States. Annals of Allergy, Asthma & Immunology, 121:5, 2018,S13.
76 Wood RA, Togias A, Sicherer SH, Shreffler WG, Kim EH, et.al., nes SM, Leung DYM, Vickery BP, Bird JA, Spergel JM, Iqbal A, Olsson J, Ligueros-Saylan M, Uddin A, Calatroni A, Huckabee CM, Rogers NH, Yovetich N, Dantzer J, Mudd K, Wang J, Groetch M, Pyle D, Keet CA, Kulis M, Sindher SB, Long A, Scurlock AM, Lanser BJ, Lee T, Parrish C, Brown-Whitehorn T, Spergel AKR, Veri M, Hamrah SD, Brittain E, Poyser J, Wheatley LM, Chinthrajah RS. Omalizumab for the Treatment of Multiple Food Allergies. N Engl J Med. 2024 Mar 7;390(10):889-899. DOI: 10.1056/NEJMoa2312382. Epub 2024 Feb 25. PMID: 38407394.
77 Perkin MR, Logan K, Marrs T, Radulovic S, Craven J, Flohr C, Lack G; EAT Study Team. Enquiring About Tolerance (EAT) study: Feasibility of an early allergenic food introduction regimen. J Allergy Clin Immunol. 2016 May;137(5):1477-1486.e8. DOI: 10.1016/j.jaci.2015.12.1322.